Social Anxiety
By Todd KashdanGeorge Mason University
Social anxiety occurs when we are overly concerned about being humiliated, embarrassed, evaluated, or rejected by others in social situations. Everyone experiences social anxiety some of the time, but for a minority of people, the frequency and intensity of social anxiety is intense enough to interfere with meaningful activities (e.g., relationships, academics, career aspirations). When a person’s level of social anxiety is excessive, social interactions are either dreaded or avoided, social cues and emotions are difficult to understand, and positive thoughts and emotions are rare, then that person may be diagnosed with social anxiety disorder (or social phobia). There are effective treatments—with both medications and psychotherapy–for this problem. Unfortunately, only a small proportion of people with social anxiety disorder actually seek treatment.
Learning Objectives
- Distinguish social anxiety from social anxiety disorder.
- Identify commonly feared social situations.
- Know the prevalence and treatment rates of social anxiety disorder.
- Understand how social anxiety influences thoughts, feelings, and behaviors.
- Identify effective treatments for social anxiety disorder.
Introduction
A public speaker waits backstage before her name is called. She visualizes what will happen in a few moments: the audience will cheer as she walks out and then turn silent, with all eyes on her. She imagines this will cause her to feel uncomfortable and, instead of standing balanced, she will lean to one side, not quite sure what to do with her hands. And when her mouth opens, instead of words, guttural sounds will emerge from a parched throat before her mind goes blank. In front of friends, family, and strangers, she is paralyzed with fear and embarrassment. Physically, in the moments leading up to the performance, she sweats, trembles, has difficulty breathing, notices a racing heartbeat, and feels nauseated. When someone asks her a question, she loses her voice or its pitch rises a few octaves. She attempts to hide her anxiety by tensing her muscles or telling herself to breathe and stay calm. Behaviorally, she seeks ways to escape the audience’s gaze (e.g., by playing a video and asking the audience questions), and she tries to get through the performance as quickly as possible (e.g., rushing off the stage). Later, she works hard to avoid similar situations, passing up future speaking opportunities.
Welcome to the often terrifying world of social anxiety.

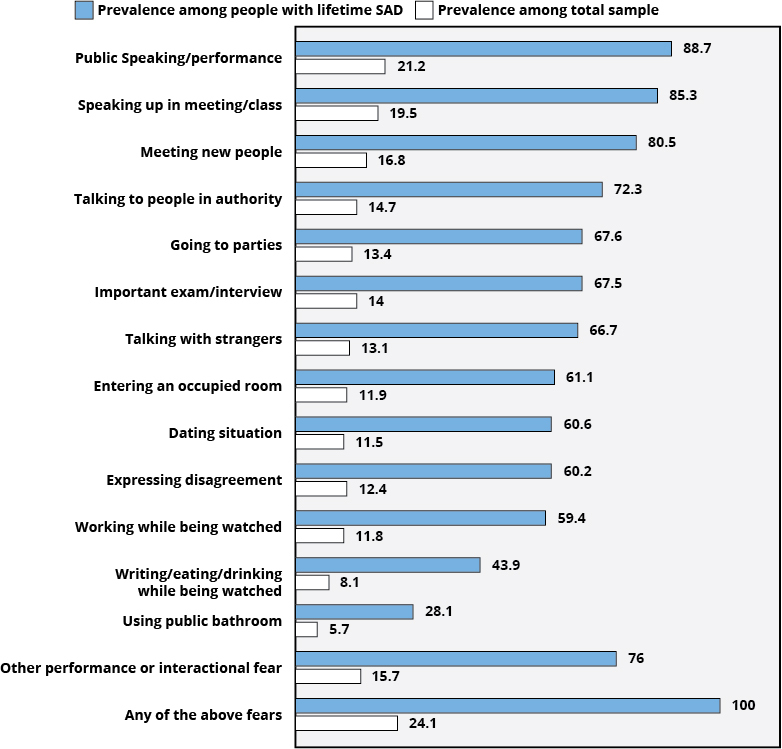
People have a fundamental need to feel like they belong and are liked, so it is painful when we feel rejected or left out by those who matter to us. In response, we often become acutely aware of the impression we make on others, and we avoid doing things that may cause others to be upset with us. Social anxiety is the excessive concern about being in social situations where scrutiny is likely. When people are socially anxious, they become overly concerned about embarrassing themselves, and they tend to reveal these signs of discomfort through sweating or blushing; they worry that their character flaws will be exposed and result in rejection. See Figure 1 for examples of situations that commonly evoke social anxiety.
The term anxiety describes a general apprehension about possible future danger, rather than a reaction to an immediate threat (i.e., fear). Nevertheless, like fear, the experience of social anxiety may involve physical, emotional, and behavioral symptoms like those described in the example above.
Nearly everyone experiences some social anxiety at one point or another. It is particularly common before performing in front of an audience or meeting new people on one’s own, and this is normal. Social anxiety provides information about the demands required of us to handle an ongoing challenge (Frijda, 1996). It lets us know that the situation is meaningful, and the impression we make on other people may be important to our social standing. Most people are able to “power through” the situation, eventually feeling more comfortable and learning that it was not as bad as expected. This is a fundamentally important point: people think that their anxiety leading up to a situation (anticipatory feelings) will only increase further in the actual situation, when, in fact, our anxiety tends to peak in the moments before a situation.
Sometimes, people experience more than the “normal” amount of anxiety. For people with excessive social anxiety, their anxiety often arises in a broader array of situations, is more intense, and does not subside as quickly. For those people, negative social outcomes are viewed as highly probable and costly, and their attention during social interactions tends to be inwardly directed (e.g., “Did my comment sound stupid? Can she tell that I’m sweating?”). This running internal commentary prevents people from focusing on the situation at hand, and even simple social interactions may become overwhelming (Bögels & Mansell, 2004).
Social Anxiety Disorder
When social anxiety and avoidance interfere with a person’s ability to function in important roles (e.g., as a student, worker, friend), the condition is called social anxiety disorder (SAD), also known as social phobia (American Psychiatric Association, 2013). In the United States, SAD affects approximately 12.1% of people in their lifetimes and 7.1% of adults in a given year (Ruscio et al., 2008). About 1 of every 4 people report at least one significant social fear in their lifetimes—most commonly, public speaking (see Figure 1). To be diagnosed with SAD, a person must report an impairing fear of multiple social situations that has persisted for at least six months. Most people with SAD fear eight or more distinct social situations such as initiating a conversation with a stranger, maintaining conversations, going on a first date, going to a work party/function, talking with an authority figure, talking in front of a group of people, and eating in front of other people (Ruscio et al., 2008).

SAD is one of the most common anxiety disorders recognized by the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM-5; APA, 2013). SAD affects men and women about equally, and the majority of people with SAD report that their fears began in early adolescence, typically around age 13 (Kessler et al., 2005). Unfortunately, this condition tends to be chronic and few people recover on their own without an intervention.
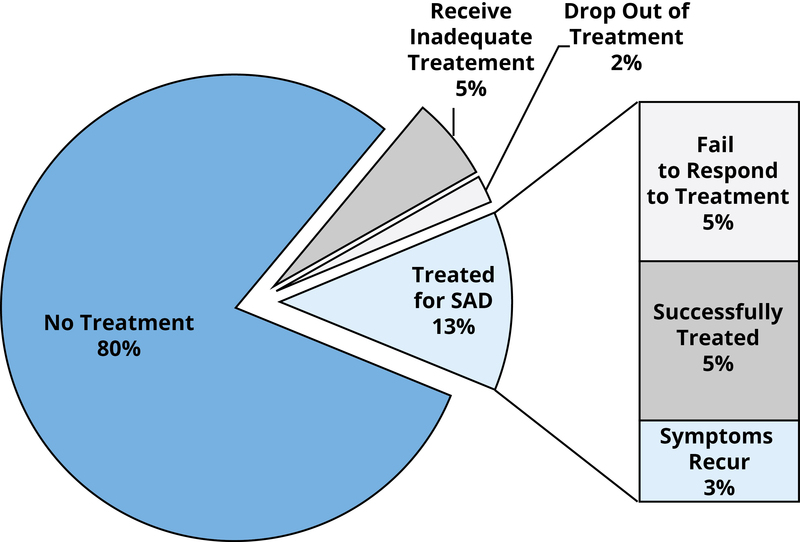
Despite the availability of effective treatments, few people seek help for their social fears (see Figure 2). In an epidemiological study, only 5.4% of people with SAD (and no other psychiatric disorders) ever received mental health treatment (Schneier, Johnson, Hornig, Liebowitz, & Weissman, 1992). There are several explanations for why people with SAD avoid treatment—for starters, the fear of being evaluated by a therapist and the stigma of seeking psychological services. Thus, the very features of the disorder may prevent a person from seeking treatment for it. Another explanation is that many physicians, teachers, parents, and peers do not believe that social anxiety disorder is a real condition and, instead, view it as nothing more than extreme shyness or inhibition. Finally, health care providers are often ill-equipped to assess SAD and may not be aware of evidence-based treatments (Kashdan, Christopher Frueh, Knapp, Hebert, & Magruder, 2006), and clients often do not know enough about social fears to discuss them with their doctors. Sadly, 60% to 80% of people with SAD suffer from symptoms for at least two decades (Ruscio et al., 2008). Thus, it is important to understand not only what social anxiety is but also what perpetuates social fears.
Fear of Evaluation
A central component of the social anxiety experience is how a person thinks about him- or herself, about others, and about social situations. According to the self-presentation theory of social anxiety (Leary & Kowalski, 1995), people feel socially anxious when they wish to make a good impression on others but doubt their ability to do so. People with excessive social anxiety are likely to view themselves as having more flaws or deficits, compared to those who rarely feel social anxiety (Clark & Wells, 1995); thus, for SAD sufferers, social interactions may seem like dangerous places where flaws can be observed and scrutinized (Moscovitch, 2009).
At first, researchers believed that the core feature of SAD was a fear of negative evaluation —being preoccupied with the possibility of being unfavorably judged or rejected by others (Watson & Friend, 1969). Recent evidence has suggested that people with SAD are actually concerned with both positive and negative evaluation. Fear of positive evaluation is the dread associated with success and public favorable evaluation, raising the expectations for subsequent social interactions. The fear of being positively evaluated is particularly relevant when a social comparison occurs, such as when a person gets a promotion at work (Weeks, Heimberg, Rodebaugh, & Norton, 2008; Weeks, Heimberg, & Rodebaugh, 2008). Both of these fears of evaluation contribute to social anxiety (Weeks, Heimberg, Rodebaugh, Goldin, & Gross, 2012).
Why might socially anxious people dread being praised? Gilbert’s (2001) evolutionary theory suggests that social anxiety is a mechanism that evolved to facilitate group cohesion. When in society there are people of different social ranks, a person lower on the social hierarchy (e.g., an entry-level employee) would experience anxiety when interacting with higher-ranking group members (e.g., bosses). Such anxiety would lead a person to display submissive behavior (e.g., avoiding eye contact) and prompt them to avoid doing anything that could cause conflict. Anything that increases social status—such as receiving a promotion or dating an attractive romantic partner—can cause tension and conflict with others of higher status. Whereas fear of negative evaluation is relevant to other psychological conditions, such as depression and eating disorders, fear of positive evaluation is unique to SAD (Fergus et al., 2009; Weeks, Heimberg, Rodebaugh, et al., 2008). Furthermore, when people are successfully treated for SAD, this fear of positive evaluation declines (Weeks et al., 2012).
Biased Attention and Interpretation
If you were to observe what people with SAD pay attention to in a social interaction, you would find that they are quick to recognize any signs of social threats. For instance, they are faster at detecting angry faces in a crowd (see Gilboa-Schechtman, Foa, & Amir, 1999). Imagine looking at the audience as you give a speech and the first faces you notice are scowling back!

At the same time, SAD sufferers’ attention is biased away from positive, rewarding information (see Taylor, Bomyea, & Amir, 2010). This means that people with SAD are unlikely to notice the smiling, nodding faces in the crowd, and they fail to pick up the subtle hints that somebody wants to spend more time with them or to be asked out on a romantic date. These interpretation and attention biases are obstacles to starting and maintaining social relationships. When you attend to only negativity, you start to believe that you are unlovable and that the world is a hostile, unfriendly place.
Complete the following sentence: “As I passed a group of people in the hall, they burst out in laughter, because . . .”
People with SAD are more likely to complete the sentence with a statement suggesting that there is something wrong with their behavior or appearance (e.g., “they thought I looked ridiculous”) as opposed to a neutral explanation (e.g., “one of them made a joke”). The problem is that when you assume people are attacking you, you feel more self-conscious and are less likely to stay in a situation and to interact with that group of people or others in the future. Our thoughts influence our behavior, and the negative interpretations and predictions of people with SAD only serve to feed their social avoidance patterns (Amir, Beard, & Bower, 2005 ).
Deficient Positive Experiences
The strongest predictor of a happy, meaningful, long-lasting life is the presence of satisfying, healthy relationships (Berscheid & Reis, 1998). Thus, the fact that people with SAD frequently avoid social interactions—even those with the potential for fun or intimacy—means that they miss out on an important source of positive experiences.
By studying people’s day-to-day experiences, researchers have discovered several positivity deficits in the lives of socially anxious people. For example, Kashdan and Collins (2010) gave participants portable electronic devices that randomly prompted them to describe what they were feeling and doing multiple times per day for several weeks. During such random assessments, socially anxious people reported less intense positive emotions (e.g., joy, happiness, calm), regardless of whether they were around other people (whereas, less anxious people report more intense positive emotions when socializing). Socially anxious people experience less frequent positive emotions even when spending time with close friends and family members (Brown, Silvia, Myin-Germeys, & Kwapil, 2007; Vittengl & Holt, 1998). In fact, even in the most intimate of situations—during sexual encounters with romantic partners—socially anxious people report less intense pleasure and less intimacy (Kashdan, Adams, et al., 2011). All of these findings highlight the vast reach of excessive social anxiety in people’s lives and how it detracts from the relationships and activities that hold the greatest promise for happiness and meaning in life (Kashdan, Weeks, & Savostyanova, 2011).

Problematic Emotion Regulation
A possible explanation for the distress and diminished positive experiences seen in SAD is that the sufferers’ ability to respond to and manage their emotions is impaired. Emotion regulation refers to how people recognize, interpret, experience, and attempt to alter emotional states (Gross, 1998). One symptom of SAD is the concern that the anxiety will be visible to others (APA, 2013). Given this concern, socially anxious people spend considerable time and effort preparing for and avoiding anxiety-related thoughts, sensations, and behaviors. They engage in safety behaviors, such as rehearsing exactly what to say in a conversation, asking questions of others to deflect attention from themselves, and holding a drink or food to have an excuse to pause before responding to a question (Clark & Wells, 1995). Because there is only so much we can pay attention to in a given moment, excessive self-focused attention detracts from a person’s ability to be mindful in a social encounter. In effect, by devoting effort to controlling emotions and minimizing the potential for rejection, a person paradoxically increases the likelihood of misunderstanding others or appearing aloof. Such encounters are also less enjoyable and possess less potential for deepening relationships.
Socially anxious people believe that openly expressing emotions is likely to have negative consequences (Juretic & Zivcic-Becirevic, 2013). In turn, they are more apt to suppress or hide their negative emotions (Spokas, Luterek, & Heimberg, 2009) and avoid anything that is distressing (Kashdan, Morina, & Priebe, 2009). Emotion suppression is often ineffective: the more we try not to think about something, the more we end up thinking about it (Richards & Gross, 1999). Unfortunately, people with SAD report being less skilled at using more effective emotion regulation strategies, such as finding alternative, constructive ways of thinking about a situation (Werner, Goldin, Ball, Heimberg, & Gross, 2011).
Socially anxious people also respond to positive emotions in an unexpected way. Whereas most people not only enjoy positive emotions but also seek them out and attempt to savor them, socially anxious people often fear intense positive emotions (Turk, Heimberg, Luterek, Mennin, & Fresco, 2005). When positive emotions arise, just like negative emotions, SAD sufferers make efforts to suppress them (Eisner, Johnson, & Carver, 2009; Farmer & Kashdan, 2012). Why downplay positive emotions? It is possible that avoiding public displays of positive emotions is another way that people with SAD can avoid scrutiny (e.g., not laughing because others might not find a joke funny) and prevent the wrath of powerful others (e.g., not expressing excitement about a personal triumph because others might be envious) (Weeks et al., 2008). A recent study sampled the day-to-day social interactions of people with and without SAD to uncover what distinguishes these two groups. What the researchers found was that the amount of social anxiety felt during social interactions was less important in distinguishing people with SAD from healthy adults than the intense effort put into avoid feeling anxious and infrequent positive emotions when spending time with other people (Kashdan et al., 2013).
The ego depletion model (Muraven & Baumeister, 2000) proposes that people have a limited capacity for physical and mental self-control (e.g., physical endurance, attention). When we perform tasks that require significant effort and energy (e.g., suppressing emotions), we deplete these self-control resources, leaving us with less capacity to focus on subsequent tasks or to make good decisions (Vohs, Baumeister, & Ciarocco, 2005). When depleted or mentally exhausted, we tend to opt for whatever is immediately rewarding as opposed to pursuing meaningful goals (Hayes, Luoma, Bond, Masuda, & Lillis, 2006). For socially anxious people, what is immediately rewarding tends to be escaping or avoiding social situations in order to minimize the potential for unpleasant feelings. In other words, the way people with high social anxiety control their emotions not only makes their social situations less pleasant in the moment but also limits their capacity for pursuing rewarding opportunities afterward. Consistent with this, Farmer and Kashdan (2012) demonstrated that over the course of two weeks, when socially anxious people used more emotion suppression, they experienced fewer pleasant social events and less intense positive emotions on the following day. Taken together, this research suggests that socially anxious people respond to their emotions in ways that have far-reaching effects on their well-being, likely maintaining fears associated with social anxiety.
Treatments
Although SAD tends to be a chronic condition if left untreated (Wittchen, Fuetsch, Sonntag, Müller, & Liebowitz, 2000), the good news is that there are effective treatments that reduce social fears. Currently, there are two gold-standard treatments for SAD: cognitive behavioral therapy (CBT) and pharmacotherapy (Gould, Buckminster, Pollack, & Otto, 1997). The frontrunner among psychotherapy options, CBT, is an approach mental health professionals (e.g., licensed clinical psychologists) use to help people with SAD learn to think, behave, and feel differently so that they can feel more comfortable in social situations and improve their quality of life (Heimberg & Becker, 2002).
The most effective strategy to treat SAD is exposure (Feske & Chambless, 1995)—where clients repeatedly confront their feared situations without the use of safety behaviors, starting with situations that are only slightly anxiety provoking (e.g., imagining a conversation with an attractive stranger) and gradually working their way up to more frightening situations (e.g., starting conversations with trained actors during therapy sections). Additional exposures are then assigned between sessions so that people can experiment with feared situations in their daily lives (e.g., saying hello to a passing pedestrian). As another example, someone who avoids riding elevators due to fear of interacting with other riders might start out by taking an elevator during off-peak hours, then during popular times, and then practicing talking with a stranger while riding an elevator, and so on. After taking part in these exposures, people learn that feared social situations are not as probable or dangerous as previously believed.

Cognitive techniques form the other component of CBT. These are strategies therapists use to help people develop more realistic and helpful thoughts and expectations about social situations. For example, people with SAD often have unrealistic beliefs that contribute to anxiety (e.g., “Everyone can see that I’m sweating”). The therapist helps them challenge such thoughts and develop more helpful expectations about situations (e.g., from “If I pause while speaking, then everyone will think I’m stupid” to “It is OK to pause; the silence may seem longer to me than to others”). These techniques are most effective in combination with behavioral techniques that help clients test out some of their assumptions in real situations (Taylor, 1996). For instance, a behavioral experiment might involve giving a cashier the wrong change (making a mistake), to test whether the feared consequence (“the cashier will laugh at me”) actually arises and, if so, whether it is as painful as expected.
Pharmacotherapy for SAD involves using medications to reduce people’s anxiety level so that they are able to stop avoiding situations and enjoy a better quality of life. The current first-line prescribed medications are selective serotonin re-uptake inhibitors (SSRIs), such as escitalopram, paroxetine, and sertraline, as well as serotonin norepinephrine reuptake inhibitors (SNRIs) like venlafaxine (Bandelow et al., 2012). Both of these medications are typically used as antidepressants that act on the neurotransmitter serotonin, which plays a big role in how the amygdala responds to possibly threatening information. SNRIs also act on norepinephrine at higher doses. These medications have few side effects and also are likely to improve symptoms of other anxiety or depression symptoms that often co-occur with SAD. Other classes of medications with some evidence of helpfulness for SAD symptoms include benzodiazepines and monoamine oxidase inhibitors, though these medications often produce a number of negative side effects (Blanco, Bragdon, Schneier, & Liebowitz, 2013).
Both approaches—CBT and medications—are moderately helpful at reducing social anxiety symptoms in approximately 60% of clients; however, the majority of people with SAD do not fully remit, and many experience a return of symptoms after treatment ends (Fedoroff & Taylor, 2001). Notably, CBT tends to have more lasting effects, and there is some modest evidence for possible added benefit when combining medications with psychotherapy (Blanco et al., 2010). It is obvious, though, that existing treatments are insufficient.
Current recommended treatments may not address some of the deficits discussed earlier. Specifically, people may avoid fewer social situations, but they might still have fewer, less intense positive life experiences. Researchers are constantly improving available treatments via new techniques and medications. Some new developments in the treatment of SAD include the encouragement of mindful awareness (vs. self-focus) and acceptance (vs. avoidance) of experiences (Dalrymple & Herbert, 2007; Goldin & Gross, 2010). As new treatments develop, it will be important to see whether these treatments not only improve SAD symptoms but also help sufferers achieve greater happiness, meaning in life, and success.
Conclusions
In this module, we discussed the normal experience of social anxiety as well as the clinically impairing distress suffered by people with SAD. It is important to remember that nearly every psychological experience and characteristic you will read about exists on a continuum. What appears to distinguish people with SAD from healthy adults is not the presence of intense social anxiety but the unwillingness to experience anxious thoughts, feelings, and sensations, and the immense effort put into avoiding this discomfort. Other problems linked to excessive social anxiety include infrequent positive events, diminished positive experiences, and a tendency to view benign and even positive social situations as threatening. Together, these symptoms prevent people from initiating and maintaining healthy social relationships, and lead to deficient well-being. When social fears become overwhelming, it is important to remember that effective treatments are available to improve one’s quality of life.
Outside Resources
- Institution: Andrew Kukes Foundation for Social Anxiety
- http://akfsa.org/
- Institution: Anxiety and Depression Association of America
- http://www.adaa.org/
- Video: Social Anxiety Documentary - Afraid of People
- Web: CalmClinic
- http://www.calmclinic.com/
- Web: Which Celebrities Suffer with Social Anxiety?
- https://www.verywell.com/which-celebrities-suffer-with-social-anxiety-3024283
Discussion Questions
- What differentiates people who are shy from those with social anxiety disorder?
- Because the most effective treatment for social anxiety disorder is exposure to feared situations, what kinds of exposures would you devise for someone who fears talking in front of an audience? Engaging in small talk? Writing or eating in front of others? Speaking up in a small group? Talking to strangers?
- Why might social anxiety disorder typically begin in late childhood/early adolescence?
- How does culture influence fears of negative and positive evaluation? After all, social groups differ in their adherence to a vertical social hierarchy.
- What may be some reasons people with severe social anxiety might not seek or receive treatment? How would you remove these obstacles?
Vocabulary
- Amygdala
- A brain structure in the limbic system involved in fear reactivity and implicated in the biological basis for social anxiety disorder.
- Anxiety
- A state of worry or apprehension about future events or possible danger that usually involves negative thoughts, unpleasant physical sensations, and/or a desire to avoid harm.
- Cognitive behavioral therapy (CBT)
- Psychotherapy approach that incorporates cognitive techniques (targeting unhelpful thoughts) and behavioral techniques (changing behaviors) to improve psychological symptoms.
- Ego depletion
- The idea that people have a limited pool of mental resources for self-control (e.g., regulating emotions, willpower), and this pool can be used up (depleted).
- Emotion regulation
- The ability to recognize emotional experiences and respond to situations by engaging in strategies to manage emotions as necessary.
- Exposure treatment
- A technique used in behavior therapy that involves a patient repeatedly confronting a feared situation, without danger, to reduce anxiety.
- Fear of negative evaluation
- The preoccupation with and dread of the possibility of being judged negatively by others.
- Fear of positive evaluation
- The dread associated with favorable public evaluation or acknowledgment of success, particularly when it involves social comparison.
- Pharmacotherapy
- A treatment approach that involves using medications to alter a person’s neural functioning to reduce psychological symptoms.
- Safety behaviors
- Actions people take to reduce likelihood of embarrassment or minimizing anxiety in a situation (e.g., not making eye contact, planning what to say).
- Selective serotonin re-uptake inhibitors (SSRIs)
- A class of antidepressant medications often used to treat SAD that increase the concentration of the neurotransmitter serotonin in the brain.
- Serotonin norepinephrine reuptake inhibitors (SNRIs)
- A class of antidepressant medications often used to treat SAD that increase the concentration of serotonin and norepinephrine in the brain.
- Excessive anticipation and distress about social situations in which one may be evaluated negatively, rejected, or scrutinized.
- An anxiety disorder marked by severe and persistent social anxiety and avoidance that interferes with a person’s ability to fulfill their roles in important life domains.
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
- Amir, N., Beard, C., & Bower, E. (2005). Interpretation bias and social anxiety. Cognitive Therapy and Research, 29(4), 433–443. doi:10.1007/s10608-005-2834-5
- Bandelow, B., Sher, L., Bunevicius, R., Hollander, E., Kasper, S., Zohar, J., … WFSBP Task Force on Anxiety Disorders, OCD and PTSD. (2012). Guidelines for the pharmacological treatment of anxiety disorders, obsessive–compulsive disorder and posttraumatic stress disorder in primary care. International Journal of Psychiatry in Clinical Practice, 16(2), 77–84. doi:10.3109/13651501.2012.667114
- Berscheid, E., & Reis, H. T. (1998). Attraction and close relationships. In D. T. Gilbert, S. T. Fiske, & G. Lindzey (Eds.), The handbook of social psychology (4th ed., Vols. 1 and 2, pp. 193–281). New York, NY: McGraw-Hill.
- Blanco, C., Bragdon, L. B., Schneier, F. R., & Liebowitz, M. R. (2013). The evidence-based pharmacotherapy of social anxiety disorder. The International Journal of Neuropsychopharmacology, 16(01), 235–249. doi:10.1017/S1461145712000119
- Blanco, C., Heimberg, R. G., Schneier, F. R., Fresco, D. M., Chen, H., Turk, C. L., … Liebowitz, M. R. (2010). A placebo-controlled trial of phenelzine, cognitive behavioral group therapy, and their combination for social anxiety disorder. Archives of General Psychiatry, 67(3), 286–295. doi:10.1001/archgenpsychiatry.2010.11
- Brown, L. H., Silvia, P. J., Myin-Germeys, I., & Kwapil, T. R. (2007). When the need to belong goes wrong: the expression of social anhedonia and social anxiety in daily life. Psychological Science, 18, 778–782. doi:10.1111/j.1467-9280.2007.01978.x
- Bögels, S. M., & Mansell, W. (2004). Attention processes in the maintenance and treatment of social phobia: hypervigilance, avoidance and self-focused attention. Clinical Psychology Review, 24(7), 827–856. doi:10.1016/j.cpr.2004.06.005
- Clark, D. M., & Wells, A. (1995). A cognitive model of social phobia. In Social phobia: Diagnosis, assessment, and treatment (pp. 69–93). New York: Guilford Press.
- Dalrymple, K. L., & Herbert, J. D. (2007). Acceptance and commitment therapy for generalized social anxiety disorder: A pilot study. Behavior Modification, 31, 543–568. doi:10.1177/0145445507302037
- Eisner, L. R., Johnson, S. L., & Carver, C. S. (2009). Positive affect regulation in anxiety disorders. Journal of Anxiety Disorders, 23(5), 645–649. doi:10.1016/j.janxdis.2009.02.001
- Farmer, A. S., & Kashdan, T. B. (2012). Social anxiety and emotion regulation in daily life: Spillover effects on positive and negative social events. Cognitive Behaviour Therapy, 41, 152–162. doi:10.1080/16506073.2012.666561
- Fedoroff, I. C., & Taylor, S. (2001). Psychological and pharmacological treatments of social phobia: A meta-analysis. Journal of Clinical Psychopharmacology, 21(3), 311–324. doi:10.1097/00004714-200106000-00011
- Fergus, T. A., Valentiner, D. P., McGrath, P. B., Stephenson, K., Gier, S., & Jencius, S. (2009). The Fear of Positive Evaluation Scale: Psychometric properties in a clinical sample. Journal of Anxiety Disorders, 23(8), 1177–1183. doi:10.1016/j.janxdis.2009.07.024
- Feske, U., & Chambless, D. L. (1995). Cognitive behavioral versus exposure only treatment for social phobia: A meta-analysis. Behavior Therapy, 26(4), 695–720. doi:10.1016/S0005-7894(05)80040-1
- Frijda, N. H. (1996). Passions: Emotion and socially consequential behavior. In Emotion: Interdisciplinary perspectives (pp. 1–27). Hillsdale, NJ: Lawrence Erlbaum Associates, Inc.
- Gilbert, P. (2001). Evolution and social anxiety: The role of attraction, social competition, and social hierarchies. Psychiatric Clinics of North America, 24(4), 723–751. doi:10.1016/S0193-953X(05)70260-4
- Goldin, P. R., & Gross, J. J. (2010). Effects of mindfulness-based stress reduction (MBSR) on emotion regulation in social anxiety disorder. Emotion, 10(1), 83–91. doi:10.1037/a0018441
- Gould, R. A., Buckminster, S., Pollack, M. H., & Otto, M. W. (1997). Cognitive-behavioral and pharmacological treatment for social phobia: A meta-analysis. Clinical Psychology: Science and Practice, 4(4), 291–306. doi:10.1111/j.1468-2850.1997.tb00123.x
- Gross, J. J. (1998). The emerging field of emotion regulation: An integrative review. Review of General Psychology, 2(3), 271–299. doi:10.1037/1089-2680.2.3.271
- Hayes, S. C., Luoma, J. B., Bond, F. W., Masuda, A., & Lillis, J. (2006). Acceptance and commitment therapy: Model, processes and outcomes. Behaviour Research and Therapy, 44(1), 1–25. doi:10.1016/j.brat.2005.06.006
- Heimberg, R. G., & Becker, R. E. (2002). Treatment of social fears and phobias. New York, NY: Guilford Press
- Juretic, J., & Zivcic-Becirevic, I. (2013). Social anxiety, beliefs about expressing emotions and experiencing positive emotions. In F. Durbano (Ed.), New insights into anxiety disorders. Rijeka, Croatia: InTech.
- Kashdan, T. B., & Collins, R. L. (2010). Social anxiety and the experience of positive emotion and anger in everyday life: An ecological momentary assessment approach. Anxiety, Stress & Coping, 23(3), 259–272. doi:10.1080/10615800802641950
- Kashdan, T. B., Adams, L., Savostyanova, A., Ferssizidis, P., McKnight, P. E., & Nezlek, J. B. (2011). Effects of social anxiety and depressive symptoms on the frequency and quality of sexual activity: A daily process approach. Behaviour Research and Therapy, 49, 352–360. doi:10.1016/j.brat.2011.03.004
- Kashdan, T. B., Christopher Frueh, B., Knapp, R. G., Hebert, R., & Magruder, K. M. (2006). Social anxiety disorder in veterans affairs primary care clinics. Behaviour Research and Therapy, 44(2), 233–247. doi:10.1016/j.brat.2005.02.002
- Kashdan, T. B., Farmer, A. S., Adams, L. M., Ferssizidis, P., McKnight, P. E., & Nezlek, J. B. (2013). Distinguishing healthy adults from people with social anxiety disorder: Evidence for the value of experiential avoidance and positive emotions in everyday social interactions. Journal of Abnormal Psychology, 122(3), 645–655. doi:10.1037/a0032733
- Kashdan, T. B., Morina, N., & Priebe, S. (2009). Post-traumatic stress disorder, social anxiety disorder, and depression in survivors of the Kosovo War: Experiential avoidance as a contributor to distress and quality of life. Journal of Anxiety Disorders, 23, 185–196. doi:10.1016/j.janxdis.2008.06.006
- Kashdan, T. B., Weeks, J. W., & Savostyanova, A. A. (2011). Whether, how, and when social anxiety shapes positive experiences and events: A self-regulatory framework and treatment implications. Clinical Psychology Review, 31, 786–799. doi:10.1016/j.cpr.2011.03.012
- Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593–602. doi:10.1001/archpsyc.62.6.593
- Leary, M. R., & Kowalski, R. M. (1995). Social anxiety (Vol. xii). New York, NY: Guilford Press.
- Moscovitch, D. A. (2009). What is the core fear in social phobia? A new model to facilitate individualized case conceptualization and treatment. Cognitive and Behavioral Practice, 16, 123–134. doi:10.1016/j.cbpra.2008.04.002
- Muraven, M., & Baumeister, R. F. (2000). Self-regulation and depletion of limited resources: Does self-control resemble a muscle? Psychological Bulletin, 126(2), 247–259. doi:10.1037/0033-2909.126.2.247
- Richards, J. M., & Gross, J. J. (1999). Composure at any cost? The cognitive consequences of emotion suppression. Personality and Social Psychology Bulletin, 25(8), 1033–1044. doi:10.1177/01461672992511010
- Ruscio, A. M., Brown, T. A., Chiu, W. T., Sareen, J., Stein, M. B., & Kessler, R. C. (2008). Social fears and social phobia in the USA: Results from the National Comorbidity Survey Replication. Psychological Medicine, 38(1), 15–28. doi:10.1017/S0033291707001699
- Schneier, F. R., Johnson, J., Hornig, C. D., Liebowitz, M. R., & Weissman, M. M. (1992). Social phobia: Comorbidity and morbidity in an epidemiologic sample. Archives of General Psychiatry, 49(4), 282–288. doi:10.1001/archpsyc.1992.01820040034004
- Spokas, M., Luterek, J. A., & Heimberg, R. G. (2009). Social anxiety and emotional suppression: The mediating role of beliefs. Journal of Behavior Therapy and Experimental Psychiatry, 40, 283–291. doi:10.1016/j.jbtep.2008.12.004
- Taylor, C. T., Bomyea, J., & Amir, N. (2010). Attentional bias away from positive social information mediates the link between social anxiety and anxiety vulnerability to a social stressor. Journal of Anxiety Disorders, 24(4), 403–408. doi:10.1016/j.janxdis.2010.02.004
- Taylor, S. (1996). Meta-analysis of cognitive-behavioral treatments for social phobia. Journal of Behavior Therapy and Experimental Psychiatry, 27(1), 1–9.
- Turk, C. L., Heimberg, R. G., Luterek, J. A., Mennin, D. S., & Fresco, D. M. (2005). Emotion dysregulation in generalized anxiety disorder: A comparison with social anxiety disorder. Cognitive Therapy and Research, 29(1), 89–106. doi:10.1007/s10608-005-1651-1
- Vittengl, J. R., & Holt, C. S. (1998). A time-series diary study of mood and social interaction. Motivation and Emotion, 22(3), 255–275.
- Vohs, K. D., Baumeister, R. F., & Ciarocco, N. J. (2005). Self-regulation and self-presentation: Regulatory resource depletion impairs impression management and effortful self-presentation depletes regulatory resources. Journal of Personality and Social Psychology, 88, 632–657. doi:10.1037/0022-3514.88.4.632
- Watson, D., & Friend, R. (1969). Measurement of social-evaluative anxiety. Journal of Consulting and Clinical Psychology, 33, 448–457. doi:10.1037/h0027806
- Weeks, J. W., Heimberg, R. G., & Rodebaugh, T. L. (2008). The Fear of Positive Evaluation Scale: Assessing a proposed cognitive component of social anxiety. Journal of Anxiety Disorders, 22(1), 44–55. doi:10.1016/j.janxdis.2007.08.002
- Weeks, J. W., Heimberg, R. G., Rodebaugh, T. L., & Norton, P. J. (2008). Exploring the relationship between fear of positive evaluation and social anxiety. Journal of Anxiety Disorders, 22, 386–400. doi:10.1016/j.janxdis.2007.04.009
- Weeks, J. W., Heimberg, R. G., Rodebaugh, T. L., Goldin, P. R., & Gross, J. J. (2012). Psychometric evaluation of the Fear of Positive Evaluation Scale in patients with social anxiety disorder. Psychological Assessment, 24(2), 301–312. doi:10.1037/a0025723
- Werner, K., Goldin, P., Ball, T., Heimberg, R., & Gross, J. (2011). Assessing emotion regulation in social anxiety disorder: The emotion regulation interview. Journal of Psychopathology and Behavioral Assessment, 33(3), 346–354. doi:10.1007/s10862-011-9225-x
- Wittchen, H. U., Fuetsch, M., Sonntag, H., Müller, N., & Liebowitz, M. (2000). Disability and quality of life in pure and comorbid social phobia. Findings from a controlled study. European Psychiatry, 15(1), 46–58. doi:10.1016/S0924-9338(00)00211-X
- ilboa-Schechtman, E., Foa, E. B., & Amir, N. (1999). Attentional biases for facial expressions in social phobia: The face-in-the-crowd paradigm. Cognition & Emotion, 13(3), 305–318. doi:10.1080/026999399379294
Authors
 Todd KashdanDr. Todd B. Kashdan is a recognized authority on personality, well-being and social relationships. He has published more than 150 scholarly articles. In 2013 he received the American Psychological Association's Distinguished Scientific Award for Early Career Contribution to Psychology in the area of Individual Differences. His work has been featured in several media outlets, including The New York Times, The Washington Post, and the Harvard Business Review.
Todd KashdanDr. Todd B. Kashdan is a recognized authority on personality, well-being and social relationships. He has published more than 150 scholarly articles. In 2013 he received the American Psychological Association's Distinguished Scientific Award for Early Career Contribution to Psychology in the area of Individual Differences. His work has been featured in several media outlets, including The New York Times, The Washington Post, and the Harvard Business Review.
Creative Commons License



 Social Anxiety by Todd Kashdan is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. Permissions beyond the scope of this license may be available in our Licensing Agreement.
Social Anxiety by Todd Kashdan is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. Permissions beyond the scope of this license may be available in our Licensing Agreement.